Highlights from the APAC Bone Health Summit 2026
Osteoporosis continues to pose a growing and complex challenge across Asia, particularly among postmenopausal women who face unique biological, clinical, and socioeconomic risk factors. At the APAC Bone Health Summit, held on March 7, 2026, at the Westin Manila, leading experts gathered to address a critical question:
How can we optimize long-term osteoporosis management in Asian women, balancing evidence, real-world dilemmas, and patient-centered decisions?
With the theme “Long-term osteoporosis management in Asian women: Evidence, Dilemmas, Decisions,” the summit moved beyond traditional treatment paradigms and into a more nuanced discussion, one that emphasized sequential therapy, individualized treatment strategies, and practical decision-making in real-world settings.
Figure 1. Speakers and organizers of the APAC Bone Health Summit.
Osteoporosis management is shifting from static treatment to strategic sequencing.
A central theme that emerged throughout the summit was the transition from a single-drug, long-term approach to a dynamic, goal-directed treatment strategy. Professor Peter Ebeling reframed osteoporosis management not as a fixed intervention, but as a lifecycle-based process that evolves alongside the patient’s fracture risk, bone mineral density (BMD), and clinical context. This shift reflects a deeper understanding that osteoporosis is not a short-term condition, but a chronic disease requiring long-term planning and adaptability.
Treat-to-target strategies are redefining what successful treatment looks like.
Traditional thresholds such as a T-score of –2.5 are no longer viewed as sufficient universal targets. Instead, experts emphasized a treat-to-target approach that aligns treatment goals with individual patient risk. In high-risk patients, achieving a higher BMD target, such as a T-score ≥ –2.0, may be more appropriate to reduce fracture risk more effectively.
1
Key principles of this approach include
1:
- Targeting higher BMD thresholds in high-risk individuals
- Recognizing total hip BMD as a reliable predictor of fracture risk
- Guiding treatment decisions based on the distance from target rather than baseline values alone
This evolving mindset reflects a broader transformation in clinical care, where success is defined not just by treating disease, but by achieving outcomes that meaningfully reduce patient risk.
Early and aggressive treatment is critical in patients at risk of subsequent fracture.
The summit strongly underscored the importance of timely intervention, particularly in patients with recent fractures. Following a vertebral fracture, the risk of subsequent fractures is highest within the first year, reaching approximately 15%. This concept of imminent risk highlights a critical window during which effective treatment can significantly alter disease trajectory.
2
Anabolic therapies were emphasized as particularly valuable in this setting. By stimulating new bone formation, these agents provide faster and greater increases in BMD compared to antiresorptive therapies, along with improved bone microarchitecture and superior fracture risk reduction. As a result, there is growing consensus that initiating treatment with an anabolic agent offers the greatest opportunity for meaningful clinical impact.
2
Sequential therapy has become the foundation of modern osteoporosis care.
Sequential therapy, defined as the strategic use of different drug classes over time, is now recognized as a cornerstone of optimal osteoporosis management. The preferred sequence, anabolic therapy followed by antiresorptive treatment, allows clinicians to first build bone and then preserve those gains over the long term.
3
However, the summit highlighted that sequencing is not merely theoretical but has direct clinical consequences. The order in which therapies are administered can significantly influence treatment outcomes.
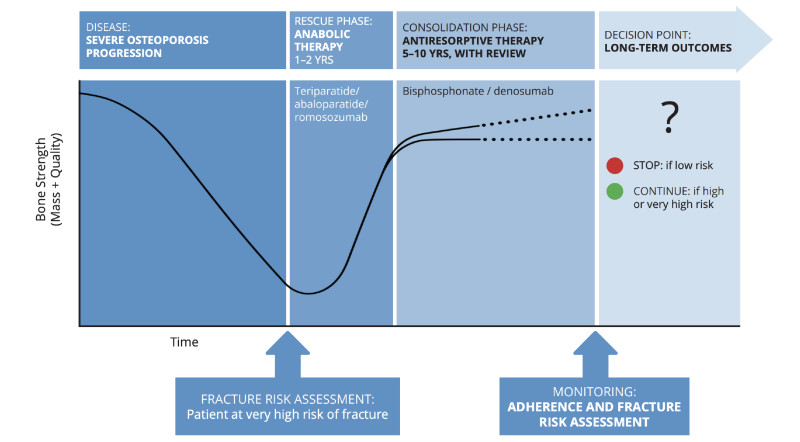
Figure 2. Proposed framework for sequential therapy: In patients with severe osteoporosis and a high imminent fracture risk identified after assessment, initiation of a bone-forming agent for 1–2 years is recommended, with duration guided by prescribing guidelines. This should be followed by a consolidation phase using antiresorptive therapy (e.g., bisphosphonates or denosumab). Ongoing monitoring, including evaluation of treatment adherence and periodic reassessment of fracture risk, is essential. Adapted from Curtis EM, et al.
Aging Clin Exp Res 2022;34:695–714.
Important sequencing considerations include:
- Starting with anabolic therapy maximizes BMD gains and fracture risk reduction
4
- Initiating treatment with antiresorptives may blunt the response to subsequent anabolic therapy, although not resulting increased fracture risk
5
- Failure to follow anabolic therapy with an antiresorptive leads to rapid loss of gains
4
These insights reinforce the importance of planning beyond treatment initiation, ensuring that transitions between therapies are deliberate and evidence-based.
Denosumab is highly effective but requires long-term commitment and planning.
Denosumab was highlighted as a potent antiresorptive agent with strong efficacy in increasing BMD and reducing vertebral, non-vertebral, and hip fractures. Its twice-yearly dosing also supports adherence, making it an attractive long-term option. However, its use introduces a critical clinical challenge.
Discontinuation of denosumab without an appropriate transition strategy can lead to rapid bone loss and an increased risk of multiple vertebral fractures, a phenomenon that has significant clinical implications. As such, denosumab therapy must always be initiated with a long-term plan in mind.
6
Key considerations include that no drug holiday is recommended with denosumab, and that long-term use (up to 10 years or more) may be required. In this context, denosumab is not simply a convenient therapy but one that demands commitment, monitoring, and careful exit planning.
6 This long-term planning can be especially important considering even elderly patients may have many years of active life to consider.
Bisphosphonates remain a cornerstone of high-risk patients, especially in Asian women.
Bisphosphonates continue to serve as the backbone of osteoporosis treatment due to their accessibility, affordability, and proven efficacy. However, the summit highlighted important ethnic considerations, particularly the increased risk of atypical femoral fractures among Asian women with prolonged use.
This risk necessitates a more cautious and individualized approach to treatment duration.
Key considerations for bisphosphonate use in Asian populations include
7:
- Optimal treatment duration is often 3–5 years
- Drug holidays may be considered in lower-risk patients
- Continued therapy is warranted in those with persistent high fracture risk
This approach reflects the need to balance long-term benefits with population-specific risks.
Ibandronic acid is being repositioned as a strategic option in sequential therapy.
Within the evolving landscape of osteoporosis treatment, ibandronic acid is gaining renewed attention. While historically considered less potent than agents such as zoledronic acid, its pharmacologic profile offers distinct advantages that make it valuable in selected clinical scenarios.
Ibandronate provides effective vertebral fracture protection and sustained improvements in BMD, particularly at the spine. Its availability in both oral and intravenous formulations allows flexibility, which can improve patient adherence and overall treatment experience.
8
Importantly, its role is now better understood within the framework of sequential therapy.
Ibandronate plays a practical role in maintenance and individualized care.
Rather than serving as a first-line therapy in very high-risk patients, ibandronate is increasingly used in maintenance or consolidation phases following anabolic treatment. In patients who have achieved significant improvements in BMD but do not require the most potent antiresorptive effect, ibandronate offers a balanced and patient-friendly option.
9
It may be particularly useful in patients who:
- Are closer to their BMD treatment targets
- Require a more tolerable or flexible regimen
- Are intolerant of more potent antiresorptive agents
- Benefit from improved adherence through less frequent dosing
Compared with other bisphosphonates, ibandronate offers several practical benefits that may improve persistence with therapy. It is associated with a lower incidence of acute-phase reactions compared to zoledronic acid, which can otherwise limit patient acceptance of intravenous treatments. Additionally, its dosing flexibility, particularly with intravenous administration, may improve adherence compared to oral bisphosphonates, where gastrointestinal side effects and strict dosing requirements often contribute to discontinuation.
9
Key practical advantages include:
- Lower incidence of acute-phase reactions compared to other IV bisphosphonates
- Improved adherence and convenience versus oral bisphosphonates
- Availability of both oral and intravenous dosing options
An additional consideration is ibandronate’s moderate bone-binding affinity. Unlike high-affinity bisphosphonates that remain in the bone matrix for prolonged periods, ibandronate allows relatively more flexibility in bone remodeling. This may be advantageous in long-term treatment planning, particularly for patients who may require future anabolic therapy. Excessive suppression of bone turnover from prior potent antiresorptive use has been shown to blunt anabolic response, and ibandronate may offer a more balanced approach in this regard.
10
Despite some limitations in the evidence backing ibandronate (along with similar agents like zoledronate) for hip and non-vertebral fractures, there is still an important role for its use in these cases, especially in the context of sequential care.
Guidance like a position statement from the American Society for Bone and Mineral Research and the Bone Health & Osteoporosis Foundation task force on goal-directed osteoporosis protection, for example, recommends the use of bisphosphonates after anabolic agents for patients close to BMD targets.
1
Additionally, real-world evidence continues to show that ibandronate is non-inferior to other bisphosphonate treatments making them a solid choice in this category.
8
Taken all together, the evidence shows that while ibandronate should not be considered a universal solution, it is still an effective and valuable option within a broader therapeutic strategy.
Individualized treatment remains the most important principle in osteoporosis care.
Throughout the summit, experts emphasized that there is no single “best” treatment for osteoporosis. Instead, optimal care requires tailoring therapy to the individual patient, taking into account a wide range of clinical and non-clinical factors.
These include:
- Fracture history and recency
- Bone mineral density and distance from target
- Age and comorbidities such as diabetes or chronic kidney disease
- Functional status and fall risk
- Patient preferences, tolerance, and likelihood of adherence
In many cases, the most effective treatment is not the most potent option, but the one that the patient can realistically continue over the long term.
Real-world constraints continue to shape treatment decisions across Asia.
Despite advances in therapy, real-world challenges such as cost, access, and healthcare infrastructure significantly influence clinical practice. In many regions, limited access to anabolic therapies necessitates reliance on antiresorptive agents, even in patients who may benefit from more aggressive strategies.
Adherence also remains a major concern, with up to half of patients discontinuing oral bisphosphonates within the first year. In this context, simplifying treatment regimens and aligning therapy with patient preferences are essential for improving outcomes.
Therapies such as ibandronate may offer advantages by:
- Reducing dosing frequency
- Improving tolerability
- Supporting long-term persistence
The BALTO II trial highlights the adherence benefits of ibandronate. 70.6% of participants in this international study expressed a preference for ibandronate over alendronate. This preference – which was motivated by convenience, lifestyle fit, and ease of long-term use – could have significant impacts on treatment adherence.
11 The availability of both oral and IV forms of ibandronate also contributes to its convenience and suitability for a range of patients.
Case-based discussions highlight the importance of adapting treatment over time.
The summit’s case discussions illustrated how osteoporosis management must evolve with changing patient risk. In moderate-risk patients without prior fractures, oral bisphosphonates remain a practical first-line option, particularly when combined with lifestyle interventions and adequate calcium and vitamin D intake. In these cases, adherence and persistence may be more critical than the specific drug chosen.
In contrast, patients who develop fractures, especially after anabolic therapy, must be reclassified as very high-risk. In such cases, immediate transition to antiresorptive therapy, particularly denosumab, is essential to preserve gains and prevent further fractures. These scenarios underscore the importance of continuous reassessment and timely adjustment of treatment strategies.
To help translate complex evidence into clinical practice, experts proposed a simplified framework:
- Build bone with anabolic therapy in high-risk patients
- Maintain gains with antiresorptive therapy
- Reassess regularly and adjust treatment accordingly
This approach provides a practical way to implement sequential therapy while keeping patient goals at the center of decision-making.
Ultimately, the best treatment is the one that works for the patient.
While advances in pharmacotherapy have expanded treatment options, success in osteoporosis management depends on more than selecting the most effective drug. It requires thoughtful sequencing, careful monitoring, and a deep understanding of the individual patient.
With a range of effective choices, physicians need to keep in mind the different roles that each drug plays in osteoporosis management, from the potential efficacy of denosumab in certain situations to the reliability and flexibility of bisphosphonates like ibandronate.
Additionally, sequential therapy provides a powerful framework for maximizing outcomes, and agents such as ibandronic acid now play an important role within this strategy when used appropriately. At the same time, therapies like denosumab offer substantial benefits but require careful long-term planning.
In the end, the management of osteoporosis in Asian women must balance evidence with experience, efficacy with safety, and ideal strategies with real-world feasibility. The best treatment is not defined by guidelines alone, but by how well it aligns with the patient’s needs, preferences, and circumstances. Achieving optimal outcomes requires a commitment to individualized, patient-centered care, where every decision is guided not just by what is possible, but by what is most appropriate for the patient in front of us.
References: 1. Cosman F, et al.
J Bone Miner Res 2024;39:1393–1405. 2. Balasubramanian A, et al.
Osteoporos Int 2019;30:79–92. Epub 2018 Nov 19.3. Sauhta R, et al.
Indian J Orthop 2023;57(Suppl 1):150–162. 4. McClung MR.
Osteoporos Sarcopenia 2018;4:11–15. 5. Chandran M. A
rch Endocrinol Metab 2022;66:724–738. 6. Kobayakawa T.
J Bone Miner Metab 2025;43:10–17. 7. Valleenukul T, et al.
Osteoporos Sarcopenia 2025;11:111–120. Epub 2025 Nov 24. 8. Alves C, et al.
Int J Clin Pharm 2024;46:357–367. Epub 2023 Dec 19. 9. Inderjeeth CA, et al.
Int J Womens Health 2014;7:7–17. 10. Nancollas GH, et al.
Bone 2006;38:617–627. 11. Hdji P, et al.
Joint Bone Spine 2008;75:303-310.