Daraxonrasib—an oral, potent RAS(ON) multi-selective, tri-complex inhibitor—demonstrates unprecedented survival benefits in individuals with previously treated metastatic pancreatic adenocarcinoma (mPDAC) in the landmark phase III RASolute 302 study.
“This study demonstrated a statistically significant improvement in overall survival (OS) in the RAS G12 population,” said Dr Brian Wolpin from the Dana-Farber Cancer Institute, Boston, Massachusetts, US, amidst a roaring applause and multiple standing ovations from a nearly 10,000-strong audience during a Plenary Session in ASCO 2026.
Primary endpoints: Survival in the RAS G12 cohort
After a median follow-up of 8.5 months, daraxonrasib doubled the median OS compared with chemotherapy (13.2 vs 6.6 months). This translated to a 60-percent reduction in the risk of death with the investigational agent than with chemo (hazard ratio [HR], 0.40; p=5.9×10-10).
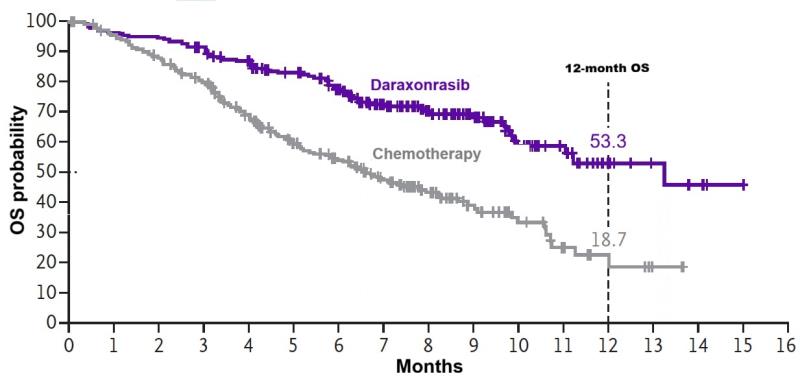
The Kaplan-Meier curves diverged as early as 2 months, and continued to do so, achieving OS probabilities of 53.3 percent with daraxonrasib and 18.7 percent with placebo at 12 months. [ASCO 2026, abstract LBA5]
OS in the RAS G12 population
Adapted fr N Engl J Med 2026;doi:10.1056/NEJMoa2605555
“This was an absolutely beautiful curve,” said discussant Dr Jennifer Knox from the Princess Margaret Cancer Centre, Toronto, Ontario, Canada, at ASCO 2026. “The curves separated early and got wider with time. I don’t think this has ever been seen in pancreatic cancer.”
Daraxonrasib also outperformed chemo in improving progression-free survival (PFS) by blinded independent central review in this subgroup (median 7.3 vs 3.5 months; HR, 0.45; p=3.2×10-9). The 6-month PFS probabilities in the respective groups were 58.7 percent and 31.7 percent.
Key secondary endpoints
The significant OS benefit with daraxonrasib was also observed in the overall population, which comprised patients with and without an identified tumour RAS mutation (median 13.2 vs 6.7 months; HR, 0.40; p=4.6×10-11; 12-month OS rates 53.2 percent vs 17.3 percent), and across all clinically relevant subgroups, with HRs ranging from 0.31 (patients with no prior 5-FU-based regimen or no liver metastases at baseline) to 0.70 (patients with other RAS G12 mutations).
The same held true for PFS in the overall population (median 7.2 vs 3.6 months; HR, 0.49; p=5.2×10-8; 6-month OS rates 56 percent vs 32.9 percent).
Daraxonrasib also significantly improved confirmed best overall response rates (ORR) compared with chemo (RAS G12: 33.2 percent vs 11.8 percent; p<0.0001; overall: 31.6 percent vs 11.2 percent; p<0.0001).
In the overall cohort, treatment with the experimental agent also led to a significant delay in time to deterioration in Global Health Status/Quality of Life in the EORTC QLQ-C30* (median 5.7 vs 2.6 months; HR, 0.60; p=0.0002) and in the EORTC QLQ-PAN26* Pain scale (median 9.2 vs 3.8 months; HR, 0.51; p<0.0001) than with chemo. According to Knox, these patient-reported outcomes (PROs) are “incredibly important findings because pancreatic cancer patients are very sick.”
Safety profile
Compared with the chemo group, the daraxonrasib group had a longer median time on treatment (6.2 vs 1.5–3.2 months) and higher median dose intensity (93.1 percent vs 65.3–95 percent).
Despite the longer time on treatment and higher dose intensities, the daraxonrasib group had fewer treatment-related adverse events (TRAEs) leading to dose reduction (36.1 percent vs 57.5 percent) and discontinuation (1.2 percent vs 11.2 percent), grade ≥3 TRAEs (43.6 percent vs 57.5 percent), and serious TRAEs (10.8 percent vs 18.7 percent).
With daraxonrasib, the most common TRAES that led to dose reduction were rash (17.4 percent) and stomatitis (6.6 percent). The three discontinuations were due to maculo-papular rash (n=2) and elevated liver function enzymes (n=1).
The most common grade ≥3 TRAEs with daraxonrasib were rash (14 percent), stomatitis (12 percent), and diarrhoea (5 percent). With chemo, the most common were haematological events, such as neutropenia (28 percent), anaemia (16 percent), and thrombocytopenia (10 percent).
No RAS-targeted Txs for PDAC
“PDAC is among the most challenging and lethal cancers, with limited therapeutic options,” Wolpin said. Furthermore, standard cytotoxic chemo regimens only provide modest benefit in previously treated mPDAC. [JAMA 2021;326:851-862; BMC Gastroenterol 2023;23:212; Cancer Treat Rev 2023;113:102502]
Excessive RAS(ON) signalling drives tumour growth across RAS-mutant and RAS wild-type PDAC, with >90 percent of tumours harbouring an activating oncogenic RAS mutation. [J Clin Oncol 2025;43:777; Cancer Cell 2017;32:185-203.e13] “There are no RAS-targeted therapies currently approved for PDAC, highlighting a substantial unmet need,” Wolpin emphasized.
In a previous phase I/II study, daraxonrasib demonstrated promising clinical activity with manageable safety in patients with previously treated advanced PDAC. [N Engl J Med 2026;394:1790-1802]
The global RASolute 302 study evaluated 500 adults (median age 66 years, 45 percent women) with mPDAC who had received one prior line of chemo in the metastatic setting. The participants were randomized 1:1 to daraxonrasib 300 mg QD or one of four standard-of-care (SoC) chemotherapy programmes**.
Approximately one-third of participants had prior pancreatectomy, 70 percent had liver metastases at baseline, and 92 percent of participants had a RAS G12 mutation (79 percent RAS G12 D/V and 13 percent other RAS G12). [N Engl J Med 2026;doi:10.1056/NEJMoa2605555]
A grand slam: Study met all endpoints
“[Taken together,] daraxonrasib met all primary and key secondary endpoints, with statistically significant and clinically meaningful improvements in OS, PFS, and ORR vs standard cytotoxic chemo in patients with previously treated mPDAC,” Wolpin said.
Daraxonrasib demonstrated a consistent treatment effect irrespective of RAS mutation status, showed a manageable safety profile with no unexpected safety findings, and improved PROs, he added.
“These results support daraxonrasib as the new SoC [in this patient setting] … We look forward to the continued evolution of RAS inhibition as an anticancer therapy and its potential to transform the treatment of pancreatic cancer,” Wolpin said in conclusion, which was again met with an overwhelming audience response.
Targeting the ‘undruggable’
“Cytotoxic chemo has been the mainstay for a long time [in PDAC], but the best median OS has stalled at approximately 1 year for the last 15 years even with all the advances in other areas of oncology,” said Knox.
There is a long and complex history of developing a drug to target the ‘undruggable’ RAS oncogene, Knox shared. “To impact pancreatic cancer, you have to target the common alleles (G12D, G12V, and G12R) and some other rare ones. The strategy must be a pan-RAS strategy, as with daraxonrasib, or an allele-specific strategy for one of the major mutations.”
RASolute 302 is an unprecedented positive trial, with survival, quality of life (QoL), and pain control being the most important endpoints, Knox emphasized.
“RAS-targeted therapy should dominate trials across the full spectrum of pancreatic cancer clinical presentations, either as monotherapy or in rational combinations, to benefit more patients, impacting survival and QoL,” Knox said.
Knox shared that the audience’s enthusiastic optimism may signify relief that “finally, we have this transformative breakthrough for pancreatic cancer.”
In the press release, ASCO Expert Dr Rachna Shroff from the University of Arizona Cancer Center, Tucson, Arizona, US, said that the findings are “landscape-changing for [mPDAC] patients with a KRAS mutation … The RAS revolution is here, and this study is proof of principle that targeting KRAS in pancreatic cancer is feasible and effective.”
*EORTC QLQ-C30/PAN26: European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire/Pancreatic Cancer Module
**Gemcitabine and nab-paclitaxel (most common); modified 5-fluorouracil (5-FU), irinotecan, leucovorin (LV), and oxaliplatin; nanoliposomal irinotecan + 5-FU/LV; LV, 5-FU, and oxaliplatin