EHA 2024: Elranatamab shows mPFS of nearly 1.5 years in heavily pretreated R/R MM
31 Oct 2024

Elranatamab monotherapy demonstrated a median progression-free survival (mPFS) of 17.2 months and median overall survival (mOS) of >2 years in heavily pretreated patients with relapsed or refractory multiple myeloma (R/R MM) who had received a median of five prior lines of therapy, with no new safety signals, according to long-term follow-up data from the MagnetisMM-3 trial presented at the 29th Congress of the European Hematology Association (EHA 2024).
Dual-target bsAb: BCMA x CD3
Patients with R/R MM often have limited therapeutic options as their disease progresses, resulting in increasingly shorter remission with every treatment line. [Blood Rev 2021:49:100808]
Elranatamab is a bispecific antibody (bsAb) targeting B-cell maturation antigen (BCMA) and CD3. It is indicated for treatment of R/R MM in patients who have received ≥3 prior therapies, including an immunomodulatory drug (IMiD), a proteasome inhibitor (PI), and an anti-CD38 antibody, and have demonstrated disease progression on the last therapy. [Nat Med 2023;29:2259-2267; Elrexfio Hong Kong Prescribing Information, March 2024]
MagnetisMM-3: Elranatamab in BCMAnaïve R/R MM
The open-label, single-arm, multicentre, phase II MagnetisMM-3 trial evaluated the efficacy and safety of elranatamab monotherapy in 123 patients with R/R MM (median age, 68.0 years; male, 55.3 percent) who had not received prior BCMA-directed therapy. [Nat Med 2023;29:2259-2267]
Heavily pretreated population
At baseline, a high proportion of patients (76.4 percent) had ≥1 poor prognostic features, including pentarefractory disease (ie, refractory to ≥2 PIs, ≥2 IMiDs and ≥1 anti-CD38 antibody; 42.3 percent), extramedullary disease (assessed by blinded independent central review [BICR]; 31.7 percent), high-risk cytogenetics (ie, t[4;14], t[14;16] or del[17p] chromosomal abnormalities; 25.2 percent), bone marrow plasma cells ≥50 percent (21.1 percent), stage III disease based on the Revised International Staging System (15.4 percent), and Eastern Cooperative Oncology Group performance status of 2 (5.7 percent).
Most patients in MagnetisMM-3 were heavily pretreated:
Deep and durable responses
Elranatamab monotherapy achieved the primary endpoint of objective response rate (ORR) as assessed by BICR at the previous data cut-off (median follow-up, 14.7 months) of the MagnetisMM-3 trial. [Nat Med 2023;29:2259-2267]
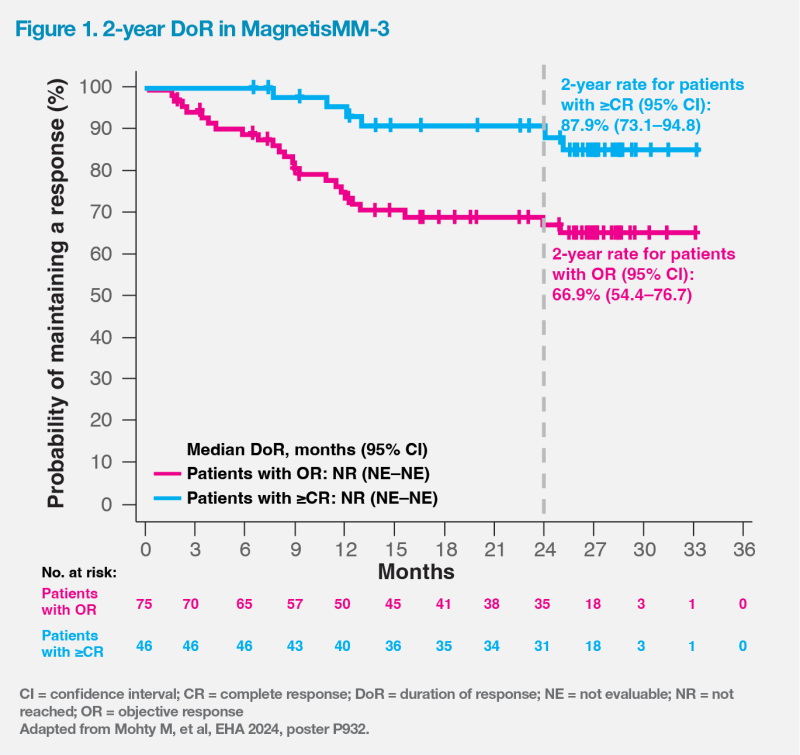
After a median follow-up of 28.4 months by reverse Kaplan-Meier method (data cut-off, 26 March 2024), elranatamab continued to demonstrate deep and durable responses in BCMA-naive patients with R/R MM. [Mohty M, et al, EHA 2024, poster P932]
ORR was high at 61.0 percent in this heavily pretreated population, despite the high proportion of patients with poor prognostic features at baseline. More than one-third (37.4 percent) of patients achieved complete response (CR) or better, with 21.1 percent achieving CR and 16.3 percent achieving stringent CR. Among evaluable patients (those with ≥CR evaluable for minimal residual disease [MRD]; n=31), 90.3 percent achieved MRD negativity at a threshold of 10-5.
Median duration of response (DoR) was not reached in patients with ≥CR or objective response. The probability of maintaining a response at 2 years was 87.9 percent (95 percent confidence interval [CI], 73.1–94.8) in patients with ≥CR and 66.9 percent (95 percent CI, 54.4–76.7) in those with objective response. (Figure 1)
Longest PFS among anti- BCMA bsAbs
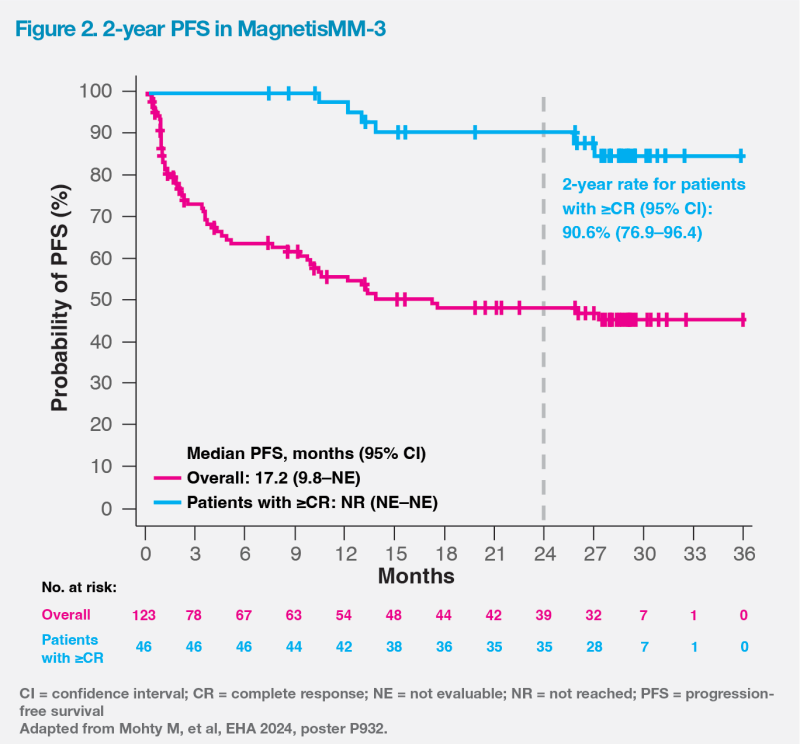
Notably, long-term follow-up results of MagnetisMM-3 demonstrated the longest reported mPFS among anti-BCMA bsAbs. [https://www.pfizer. com/news/press-release/press-release-detail/elrexfiotm-shows-median-overall-survival-more-two-years]
mPFS was 17.2 months (95 percent CI, 9.8–not evaluable [NE]), and mOS was 24.6 months (95 percent CI, 13.4–NE). These were markedly longer than those observed in triple class–refractory patients in the real-world LocoMMotion study, which reported a mPFS of 4.6 months and a mOS of 12.4 months. [Leukemia 2022;36:1371-1376; Mohty M, et al, EHA 2024, poster P932] In patients with ≥CR, mPFS was not reached, and the 2-year PFS rate was 90.6 percent (95 percent CI, 76.9–96.4). (Figure 2)
Manageable safety profile
The most common treatmentemergent adverse events (AEs) reported in MagnetisMM-3 were infections (any grade, 69.9 percent; grade 3–4, 39.8 percent), cytokine release syndrome (CRS; any grade, 57.7 percent; grade 3–4, 0 percent), and haematologic-related AEs, including anaemia (any grade, 48.8 percent; grade 3–4, 37.4 percent) and neutropenia (any grade, 48.8 percent; grade 3–4, 48.8 percent). Haematologic-related AEs were generally manageable with dose reductions or interruptions, and supportive therapies. Immune effector cell–associated neurotoxicity syndrome (ICANS) was infrequent (3.4 percent) and of grade 1–2. [Nat Med 2023;29:2259-2267]
No new safety signals were observed in the long-term follow-up. Five patients (4.1 percent) experienced secondary primary malignancies (SPMs), all of which were squamous-cell carcinomas of the skin, and all had previously received treatment with lenalidomide and stem-cell transplant. No haematologic SPMs were observed. [Mohty M, et al, EHA 2024, poster P932]
Biweekly dosing
Patients received subcutaneous elranatamab in two step-up doses (12 mg on day 1 and 32 mg on day 4), followed by a full treatment dose of 76 mg QW. After ≥24 weeks of treatment, persistent responders could switch to a Q2W dosing schedule. Importantly, the incidence of grade 3–4 AEs with Q2W dosing dropped from 58.6 to 46.6 percent without compromising efficacy. [Elrexfio Hong Kong Prescribing Information, March 2024; Nat Med 2023;29:2259-2267]