Liposarcoma (LPS) is a rare malignant tumour of adipose tissue, characterized by significant heterogeneity and limited systemic treatment options, particularly in advanced stages. At an industry-sponsored symposium, Dr Herbert Loong of the Chinese University of Hong Kong reviewed advances in systemic therapies for LPS, highlighting clinical evidence supporting the use of eribulin in second-line (2L) and later settings. Dr Olivia Chen, on behalf of the Prince of Wales Hospital sarcoma group, presented a local case of LPS treated with eribulin + lenvatinib, which demonstrated durable clinical benefit over 2 years.
LPS: Navigating a complex disease
Soft tissue sarcomas (STS) are a rare and heterogeneous group of tumours, accounting for about 1 percent of adult malignancies and comprising >80 distinct histological subtypes. Among these, LPS represents roughly one-fifth of cases. LPS can be broadly classified into four main subtypes — well-differentiated (WDLPS), dedifferentiated (DDLPS), myxoid (MLPS), and pleomorphic (PLPS) — each with distinct molecular features, clinical behaviour, and treatment sensitivity. [Oncol Res Treat 2022;45:525-543]
“Therefore, identifying LPS subtypes is important, and an accurate molecular diagnosis — using tests such as those that detect alterations in MDM2, CDK4 and DDIT3 — is essential to guide treatment decisions,” noted Loong.
Surgical resection remains the cornerstone of treatment for localized LPS. The addition of radiotherapy may improve disease control, particularly in MLPS (the most radiosensitive among the four main subtypes). Anthracycline-based systemic chemotherapy (eg, doxorubicin) is typically used as first-line (1L) therapy for patients with unresectable, advanced, or metastatic disease. For anthracycline-refractory disease, a histology-driven approach is recommended for subsequent lines of therapy, including eribulin, trabectedin, ifosfamide, and gemcitabine-based combinations. [Oncol Res Treat 2022;45:525-543; Ann Oncol 2021;32:1348-1365]
“The median overall survival [OS] of patients with advanced STS treated with doxorubicin monotherapy has improved over time — from 12.8 months in the EORTC trial [2014] to 19.7 months in the ANNOUNCE trial [2019],” said Loong. “These gains likely reflect improvements in multidisciplinary and supportive care, including granulocyte colony–stimulating factor, and the availability of more 2L and later-line treatment options.” [Lancet Oncol 2014;15:415-423; JAMA 2020;323:1266-1276]
Established 2L therapies
Trabectedin and eribulin illustrate the importance of carefully interpreting clinical trial endpoints in LPS. Although trabectedin is approved for both LPS and leiomyosarcoma (LMS), it did not meet its primary endpoint of OS in a randomized, phase III trial, despite significantly improving progression-free survival (PFS). In 518 patients with advanced LPS or LMS previously treated with anthracycline-based chemotherapy, trabectedin reduced the risk of disease progression or death by 45 percent vs dacarbazine (median PFS, 4.2 vs 1.5 months; hazard ratio [HR], 0.55; 95 percent confidence interval [CI], 0.44–0.70; p<0.001), with no significant OS benefit observed (median OS, 13.7 vs 13.1 months; HR, 0.93; p=0.49). [Yondelis US FDA Prescribing Information, December 2025, accessed 27 April 2026; J Clin Oncol 2016;34:786-793; Cancer 2019;125:2610-2620]
In contrast, eribulin demonstrated a significant OS benefit without a corresponding improvement in PFS in a phase III trial involving 452 patients with advanced LPS or LMS who had received ≥2 prior systemic regimens (inclusive of neoadjuvant and adjuvant settings), including an anthracycline. Eribulin improved OS vs dacarbazine (median OS, 13.5 vs 11.5 months; HR, 0.77; 95 percent CI, 0.62–0.95; p=0.0169), while PFS was similar between groups (median PFS, 2.6 vs 2.6 months; HR, 0.88; 95 percent CI, 0.71–1.09; p=0.23). [Lancet 2016;387:1629-1637]
Importantly, a prespecified subgroup analysis showed that the OS benefit was primarily driven by patients with LPS (median OS, 15.6 vs 8.4 months; HR, 0.51; 95 percent CI, 0.35–0.75; p<0.001), who also experienced significantly improved PFS (median PFS, 2.9 vs 1.7 months; HR, 0.52; 95 percent CI, 0.35–0.78; nominal p=0.0015). [J Clin Oncol 2017;35:3433-3439]
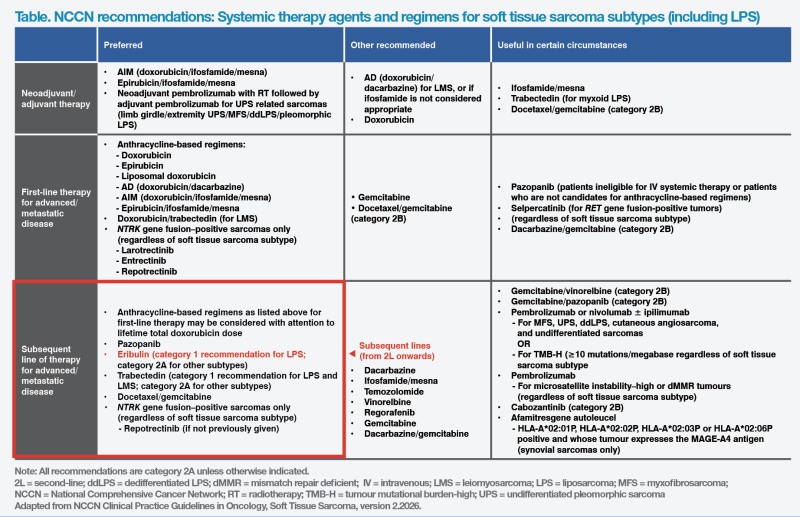
“These findings led to the incorporation of eribulin into treatment guidelines for use in 2L and later settings following anthracycline failure, with a National Comprehensive Cancer Network [NCCN] category 1 recommendation for LPS,” noted Loong. (Table) [NCCN Clinical Practice Guidelines in Oncology, Soft Tissue Sarcoma, version 2.2026]
Eribulin + lenvatinib: A rational combination
Eribulin, a microtubule inhibitor, has been shown to remodel tumour vasculature, improving perfusion and drug delivery in preclinical models*. Lenvatinib, a multi-kinase inhibitor targeting VEGFR1–3 and FGFR1–4, exerts antiangiogenic and antitumour effects. These complementary mechanisms provide a strong biological rationale for synergistic activity in combination therapy. [Cancer Sci 2014; 105:1334-1342; Cancer Sci 2017;108: 2273-2280; Vasc Cell 2014;6:18]
The phase Ib/II LEADER study evaluated the combination of eribulin (1.1 mg/m2 on days 1 and 8 of a 21-day cycle) + lenvatinib (14 mg QD) in 30 patients with advanced STS, consisting primarily of LMS (n=21) and a smaller LPS cohort (n=9). Most patients had received prior systemic therapy, although 37 percent were treatment-naïve. The objective response rate was 20 percent overall and 22 percent in the LPS subgroup. [Clin Cancer Res 2022;28:5058-5065]
“Seventy-seven percent of patients [n=23/30] showed some degree of tumour shrinkage on waterfall analysis. In sarcoma, even achieving ‘no growth’ [disease stabilization] can be considered a win,” noted Loong.
Conclusion
Eribulin has emerged as an important 2L and later therapy for LPS, demonstrating a clinically meaningful OS benefit and earning a key place in international treatment guidelines.
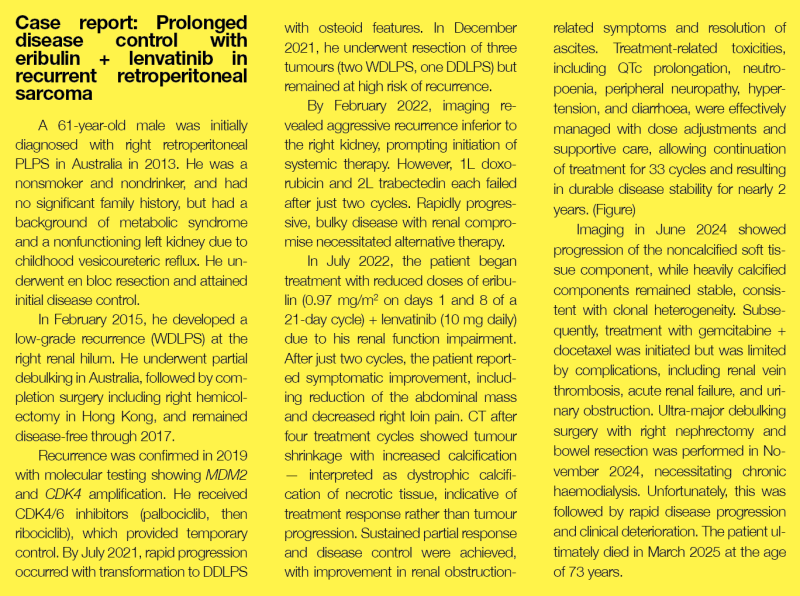
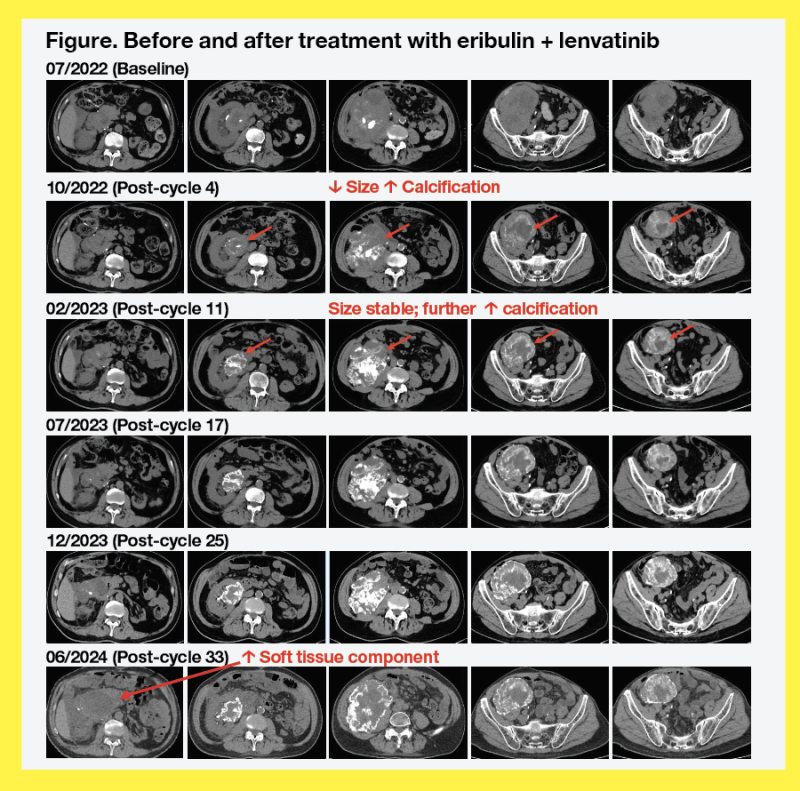
“Our case report highlights the potential of eribulin + lenvatinib to achieve prolonged disease control in selected patients. With optimal sequencing of surgery and systemic therapy, guided by a multidisciplinary approach and supported by proactive toxicity management, this combination led to nearly 2 years of disease control, delayed dialysis, reduced symptoms, and preserved quality of life,” noted Chen.
These findings reinforce the importance of individualized, multidisciplinary care and support the role of eribulin-based strategies in improving outcomes in advanced LPS.
*These findings are based on experiments in animal models.
The above editorial is for medical education purposes, supported by Eisai (HK) Co. Ltd.
HK-HL-21-001 (June 2026)