Finerenone significantly reduces albuminuria vs placebo and maintains a manageable safety profile in patients with type 1 diabetes (T1D) and chronic kidney disease (CKD) receiving background therapy with renin-angiotensin-aldosterone system inhibitors (RAASi), the phase III FINE-ONE trial has shown. These findings represent an important step forward since RAASi were introduced for renoprotection in T1D more than 30 years ago.
FINE-ONE trial design
The phase III, international, prospective, double-blind, randomized FINE-ONE trial included 242 adults with T1D and CKD (estimated glomerular filtration rate [eGFR], 25–<90 mL/min/1.73 m2) who had albuminuria (urinary albumin-to-creatinine ratio [UACR], 200–<5,000 mg/g [20–<500 mg/mmol]) and were on a stable dose of an angiotensin-converting enzyme inhibitor or angiotensin-receptor blocker for ≥4 weeks prior to screening. [N Engl J Med 2026;394:947-957]
The patients were randomized 1:1 to receive the nonsteroidal mineralocorticoid receptor antagonist (MRA), finerenone (10 or 20 mg/day, depending on eGFR*), or a matching placebo. Baseline characteristics were well balanced between participants in the finerenone group (n=120; mean age, 51.3 years; male, 65.8 percent; median baseline UACR, 574.6 mg/g [57.46 mg/mmol]; mean eGFR, 59.0 mL/min/1.73 m2) and the placebo group (n=122; mean age, 51.9 years; male, 64.8 percent; median baseline UACR, 506.4 mg/g [50.64 mg/mmol]; mean eGFR, 58.8 mL/min/1.73 m2).
The primary efficacy outcome was the relative change in UACR over a 6-month period. Exploratory efficacy outcomes included changes in UACR from baseline to months 3 and 6, and reductions of ≥30 percent and ≥50 percent in UACR from baseline at month 6 (end of the treatment period).
Finerenone reduces albuminuria
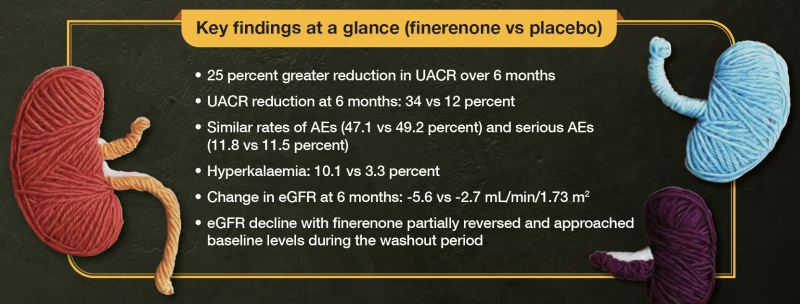
Primary outcome results showed a 25 percent greater reduction in UACR with finerenone vs placebo (least-squares [LS] geometric mean ratio for finerenone vs placebo, 0.75; 95 percent confidence interval [CI], 0.65–0.87; p<0.001) over 6 months. [N Engl J Med 2026;394:947-957]
Geometric mean change in UACR from baseline over a 6-month period was -34 percent (LS geometric mean ratio to baseline, 0.66; 95 percent CI, 0.60–0.73) in the finerenone group, compared with -12 percent (LS geometric mean ratio to baseline, 0.88; 95 percent CI, 0.79–0.98) in the placebo group.
“These effects appeared to be similar across subgroups of participants with the lowest eGFR or highest UACR – participants who are at very high risk of adverse kidney and cardiovascular [CV] outcomes,” the investigators reported.
Exploratory subgroup analysis of the primary outcome indicated significant and generally consistent benefit of finerenone vs placebo in patients with eGFR of <45 mL/min/1.73 m2 (LS geometric mean ratio, 0.74; 95 percent CI, 0.57–0.97) or 45–<60 mL/min/1.73 m2 (LS geometric mean ratio, 0.67; 95 percent CI, 0.51–0.89), and those with UACR of <300 mg/g (<30 mg/mmol) (LS geometric mean ratio, 0.71; 95 percent CI, 0.54–0.93) or 300–1,000 mg/g (30–100 mg/mmol) (LS geometric mean ratio, 0.72; 95 percent CI, 0.58–0.89). However, the benefit did not reach statistical significance in patients with eGFR ≥60 mL/min/1.73 m2 (LS geometric mean ratio, 0.82; 95 percent CI, 0.67–1.00) or UACR >1,000 mg/g (>100 mg/mmol) (LS geometric mean ratio, 0.91; 95 percent CI, 0.70–1.18).
A significant and generally consistent benefit of finerenone vs placebo on the primary outcome was also observed across subgroups of patients with serum potassium levels of 4.0–4.8 mmol/L (LS geometric mean ratio, 0.78; 95 percent CI, 0.65–0.92) or >4.8 mmol/L (LS geometric mean ratio, 0.69; 95 percent CI, 0.52–0.91), systolic blood pressure of <130 mm Hg (LS geometric mean ratio, 0.75; 95 percent CI, 0.59–0.94) or ≥130 mm Hg (LS geometric mean ratio, 0.78; 95 percent CI, 0.66–0.93), HbA1c of ≤7.5 percent (LS geometric mean ratio, 0.80; 95 percent CI, 0.66–0.98) or >7.5 percent (LS geometric mean ratio, 0.76; 95 percent CI, 0.62–0.93), and in male (LS geometric mean ratio, 0.78; 95 percent CI, 0.65–0.92) and female (LS geometric mean ratio, 0.74; 95 percent CI, 0.58–0.94) patients.
At 6 months, 54.3 percent of patients in the finerenone group had ≥30 percent reduction in UACR from baseline, while 28.4 percent had ≥50 percent reduction. In the placebo group, the respective rates were 32.7 and 21.8 percent.
No new safety signals
The safety findings of the FINE-ONE trial were consistent with those of previous studies of finerenone. [N Engl J Med 2026;394:947-957; N Engl J Med 2026;394:1019-1020]
Similar rates of adverse events (AEs; 47.1 vs 49.2 percent) and serious AEs (11.8 vs 11.5 percent) were reported in the finerenone vs placebo group. AEs and serious AEs leading to permanent discontinuation of the trial regimen were infrequent, occurring in 2.5 vs 2.5 percent and 2.5 vs 0.8 percent of patients, respectively.
Hyperkalaemia, the most common AE, was reported in 10.1 vs 3.3 percent of patients in the finerenone vs placebo group. In the finerenone group, 1.7 percent of patients discontinued treatment due to hyperkalaemia.
“Finerenone caused an acute reduction in eGFR after 1 month, and the effect was maximal at 6 months. This effect reversed in part during the 30-day washout period,” the investigators noted.
At 6 months, change in eGFR was -5.6 mL/min/1.73 m2 in the finerenone group vs -2.7 mL/min/1.73 m2 in the placebo group (difference, -2.9 mL/min/1.73 m2; 95 percent CI, -5.1 to -0.7). During the washout period from month 6 (end of treatment period) to follow-up (30 days after the last dose of finerenone or placebo), eGFR values in the finerenone group approached baseline levels. Of note, UACR increased during this washout period in the finerenone group, but not in the placebo group.
“We speculate that this finding [of acute decline in eGFR] is consistent with haemodynamic glomerular changes with finerenone, similar to those reported in persons with type 2 diabetes [T2D] and CKD and with other therapies used for kidney disorders,” the investigators wrote. [Kidney Int 2025;108:136-144; Int J Mol Sci 2022;23:9243]
An important step forward after 3 decades
RAASi were introduced for renoprotection in patients with T1D based on a randomized controlled trial of captopril vs placebo published in 1993. [N Engl J Med 2026;394:947-957; N Engl J Med 1993;329:1456-1462]
Although newer therapies, such as sodium-glucose cotransporter 2 inhibitors (SGLT2i), the nonsteroidal MRA finerenone, and the glucagon-like peptide-1 receptor agonist semaglutide, have become available for managing kidney and CV disease in patients with T2D and CKD, these agents have not been evaluated in rigorous clinical outcome trials in patients with T1D and CKD. [Diabetes Care 2025;48(Suppl 1):S239-S251]
“We have waited for 30 years since captopril’s trial for another therapy to delay kidney disease progression and reduce CV events in adults with T1D and diabetic kidney disease [DKD],” wrote Dr Aleksandra Kukla and Dr Marie C Hogan of the Department of Medicine, Mayo Clinic, Rochester, Minnesota, US, in an accompanying editorial. [N Engl J Med 2026;394:1019-1020]
“The FINE-ONE trial represents an important step toward better treatments for kidney disease in patients with T1D, particularly those with albuminuria,” they continued. “The trial is promising, but a larger, longer trial designed to show sustained kidney function benefit with broader eligibility may be required before integration into practice can occur.”
Meanwhile, an ongoing phase III trial is evaluating the efficacy and safety of sotagliflozin (an SGLT2i) vs placebo in delaying kidney function decline in patients with T1D and DKD. The primary outcome is eGFR at the end of an 8-week washout period following a 3-year treatment period. [NCT06217302]
*Initiated at 20 mg/day if screening eGFR was ≥60 mL/min/1.73 m2, and at 10 mg/day if screening eGFR was 25–<60 mL/min/1.73 m2. Dose increase from 10 mg/day to the target dose of 20 mg/day permitted from 1 month onwards in participants with serum potassium levels ≤4.8 mmol/L and a decrease in eGFR of <30 percent below the value at the last visit. Dose reduction was allowed at any time for safety reasons.