Case 1: Switching from aflibercept 2 mg to 8 mg in nAMD
History, initial treatment and response
A 53-year-old female presented on 11 March 2024 with a 2-month history of distorted vision and marked visual impairment in her left eye (OS). Her relevant treatment history included radial keratotomy. Baseline OS visual acuity (VA) was counting fingers.
The patient initially presented to a public hospital, where assessment revealed choroidal neovascularization (CNV) with macular oedema. She was diagnosed with neovascular age-related macular degeneration (nAMD) and treatment with anti-vascular endothelial growth factor (anti-VEGF) agents was recommended. However, because of difficulties in scheduling frequent appointments for anti-VEGF treatment administration at the public hospital, she sought consultation with us.
The patient received two monthly consecutive intravitreal (IVT) injections of aflibercept 2 mg at our centre in March and April 2024, and two additional nonconsecutive doses at the public hospital over the following 9 months.
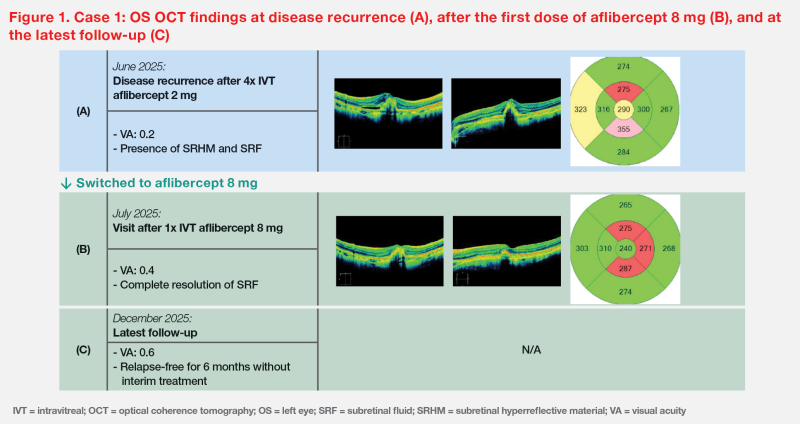
On 6 June 2025, 4 months after her last injection, the patient returned with recurrent disease. Optical coherence tomography (OCT) showed subretinal hyperreflective material (SRHM) and subretinal fluid (SRF). Central retinal thickness (CRT) was 290 μm, and VA dropped to 0.2 (20/100). (Figure 1A)
Aflibercept 8 mg treatment and response
On 10 June 2025, the patient was switched to IVT aflibercept 8 mg.1 In July 2025, 1 month after the first IVT injection of aflibercept 8 mg, her OS VA improved from 0.2 (20/100) to 0.4 (20/50). OS OCT showed complete resolution of SRF and a reduction of CRT from 290 to 240 μm. (Figures 1A and 1B)
She tolerated the treatment well, with no increase in intraocular pressure (IOP) or any other adverse events (AEs).
Last seen in December 2025, 6 months after the first injection of aflibercept 8 mg, her OS VA further improved to 0.6 (approximately 20/33) despite no interim treatment. (Figure 1C)
Case 2: Switching from faricimab to aflibercept 8 mg in PCV
History, presentation and prior treatments
A 62-year-old male presented in July 2024 with a 1-year history of OS blurred vision. In addition to bilateral cataract, he had dry AMD OS without progression to nAMD and pigment epithelial detachment (PED) OS. He underwent phacoemulsification for cataract, after which his OS VA improved from 0.5 (50/100) to 0.8 (20/25).
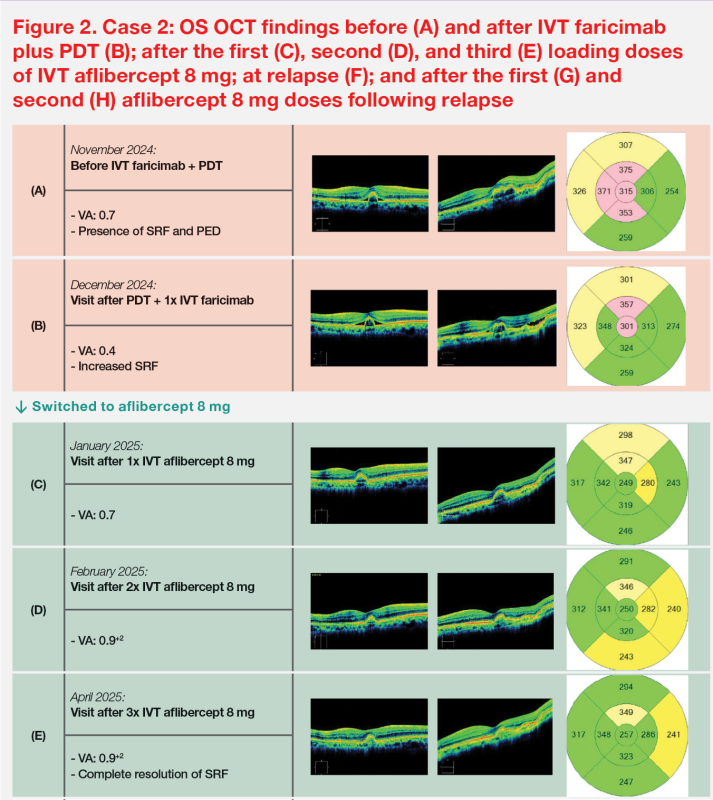
On 8 October 2024, he reported daily photopsia lasting several hours. A large polyp was observed. OS OCT in November 2024 showed SRF and a narrow, peaked PED. (Figure 2A) OS fundus fluorescein angiography and indocyanine green angiography in December 2024 showed polyps with a slow leak. The patient was diagnosed with polypoidal choroidal vasculopathy (PCV). His VA was 0.7 (approximately 20/28).
On 3 December 2024, the patient was treated with a combination of photodynamic therapy (PDT) and faricimab 6 mg. However, 3 weeks after the combination treatment was initiated, his VA deteriorated from 0.7 (approximately 20/28) to 0.4 (20/50), and OS OCT showed increased SRF. (Figures 2A and 2B)
Aflibercept 8 mg treatment and response
In view of suboptimal treatment outcomes, the patient was switched to IVT aflibercept 8 mg on 31 December 2024. He received the second dose on 28 January 2025 and the third dose on 25 February 2025.1 He tolerated the treatment well and did not experience any AEs.
His VA returned to 0.7 (approximately 20/28) after the first IVT injection of aflibercept 8 mg and further improved to 0.9+2 (approximately 20/21) after the second dose. VA was maintained at 0.9+2 (approximately 20/21) after the third loading dose of aflibercept 8 mg. Additionally, OS OCT in April 2025 showed complete resolution of SRF. (Figures 2C–2E)
Due to injection anxiety, the patient opted for a PRN dosing schedule after three loading doses. OCT was performed regularly in mainland China, and he attended follow-up visits at our centre every 1–2 months.
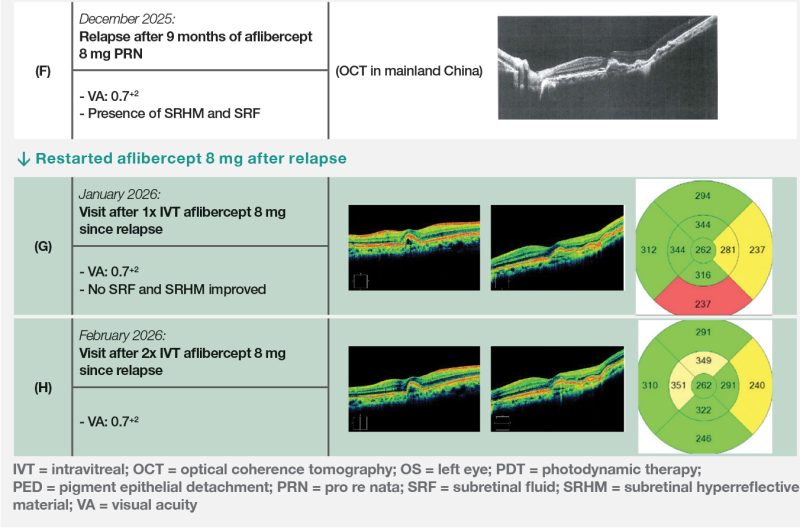
On 2 December 2025, 9 months after the last injection, the patient experienced disease recurrence: VA worsened to 0.7+2 (15/20), and OCT showed SRHM and SRF. (Figure 2F) Therefore, aflibercept 8 mg was restarted after relapse.
In January 2026, 1 month after the first dose of IVT aflibercept 8 mg for treatment of relapse, OCT OS revealed no SRF and improved SRHM. (Figure 2G) He tolerated aflibercept 8 mg well and did not experience any AEs.
Last seen on 3 February 2026, the patient’s latest VA was maintained at 0.7+2 (15/20). (Figure 2H) After discussion with the patient, a treat-and-extend (T&E) dosing schedule was decided to be followed to optimize treatment outcomes.
Discussion
Aflibercept 8 mg has been available in Hong Kong for a year. My clinical experience with this new formulation is consistent with the results of the double‑blind, randomized, phase III PULSAR trial in 1,009 patients with treatment-naïve nAMD.2
In PULSAR, following three initial monthly doses, aflibercept 8 mg demonstrated a superior drying effect in the retinal centre subfield (63 vs 52 percent; p=0.0002) at week 16 vs aflibercept 2 mg Q8W.2 Patients who completed the main phase of PULSAR through 96 weeks were eligible to an optional 1-year open-label extension through week 156. From week 96, patients originally assigned to the aflibercept 2 mg Q8W group were switched to aflibercept 8 mg Q12W (2→8 mg), and patients originally assigned to aflibercept 8 mg groups continued to receive treatment at their last assigned dosing interval.3
At week 156, the 2→8 mg group (n=208) and 8 mg group (n=417) showed a least-squares mean change from baseline in best-corrected VA (BCVA) of +4.6 and +3.4 letters and CRT of -145 and -148 μm, respectively. On average, BCVA and CRT improvements at week 96 were largely maintained through week 156.3
Similar findings were noted in both of our cases after switching to aflibercept 8 mg. In Case 1, the patient with nAMD switched from aflibercept 2 mg to aflibercept 8 mg upon disease progression, which led to improvement in VA from 0.2 to 0.6 and dry retina after a single dose of aflibercept 8 mg. (Figure 1A–1C) In Case 2, the patient with PCV switched to aflibercept 8 mg due to suboptimal treatment response with faricimab and PDT, leading to a rapid drying effect on the retina, while his VA improved from 0.4 to 0.9+2 after three loading doses. (Figures 2A–2E) Upon relapse, this patient achieved a rapid drying effect of central retina immediately after the first dose of aflibercept 8 mg. (Figures 2F–2H)
In PULSAR, among patients who completed week 156, the last assigned dosing interval was ≥Q12W, ≥Q16W, and ≥Q20W in 78, 42, and 16 percent in the 2→8mg group, respectively, and ≥Q12W, ≥Q16W, ≥Q20W, and Q24W in 77, 58, 40, and 24 percent, respectively, in the 8 mg group.3,4
Notably, proactive T&E dosing of aflibercept generally provides better visual outcomes than PRN dosing in both nAMD and PCV, as PRN dosing may be associated with risk of vision loss from delayed treatment.5-7 In my opinion, as the two patients demonstrated a long relapse-free duration on PRN dosing schedule (Case 1, ≥6 months; Case 2, ≥9 months), they are likely to achieve Q24W dosing interval with aflibercept 8 mg T&E regimen, with as few as 2 injections per year.
The safety profile of aflibercept 8 mg was comparable to that of aflibercept 2 mg, with no new safety signals identified in PULSAR over 156 weeks.2,4 The proportion of patients with IOP >35 mm Hg at any timepoint was comparable between treatment groups at 96 weeks.8 However, a few of my patients with severe glaucoma experienced elevated IOP after aflibercept 8 mg. In such cases, injecting aflibercept 2 mg may be considered.
Both aflibercept 8 mg and faricimab are excellent treatment options for nAMD and PCV. So far, in our centre’s clinical experience, nearly all patients responded to aflibercept 8 mg; however, occasionally there are patients who do not respond to other agents such as faricimab. There are currently no markers to predict nonresponse to anti-VEGF agents. In cases of nonresponse after one or more doses of a certain anti-VEGF agent, as illustrated in Case 2, I would consider switching to aflibercept 8 mg. These clinical observations suggest excellent consistency of response with aflibercept 8 mg, which increases my confidence when prescribing it to anti‑VEGF–experienced patients.
After 1 year of real-world experience, including the two cases above, I confidently use aflibercept 8 mg as first-line treatment in patients with nAMD and PCV.
References:
- Eylea 8 mg Pre-filled Syringe Prescribing Information.
- Lancet 2024;403:1141-1152.
- Lai YY, et al, ARVO 2025.
- Wong TY, et al, Macular Society 2025.
- Asia Pac J Ophthalmol (Phila) 2021;10:507-518.
- Graefes Arch Clin Exp Ophthalmol 2019;257:1889-1895.
- Rosenberg D, et al, ARVO 2021.
- Ophthalmology 2026;133:39-50.
The editorial is supported by the industry for educational purposes.
PP-EYL_8mg-HK-0158-1