Presentation, medical history and initial treatment
A 63-year-old man with hypertension, chronic kidney disease (CKD), and ischaemic heart disease previously treated with percutaneous coronary intervention presented to our clinic in January 2024. He was under the care of another nephrologist. At presentation, he was taking only antihypertensives and aspirin.
Laboratory tests showed serum creatinine level >500 μmol/L, urea at 36 mg/dL, estimated glomerular filtration rate of 6–7 mL/min/1.73 m², and haemoglobin (Hb) level at 8.5 g/dL, while serum iron level was normal. The patient was diagnosed with renal failure and started on twice-weekly haemodialysis in the same month. At the same time, long-acting erythropoietin-stimulating agent (ESA), darbepoetin alfa, 120 μg Q4W was initiated to treat his renal failure–associated anaemia. He responded to this initial treatment, with Hb level normalizing over the next few months. (Figure)
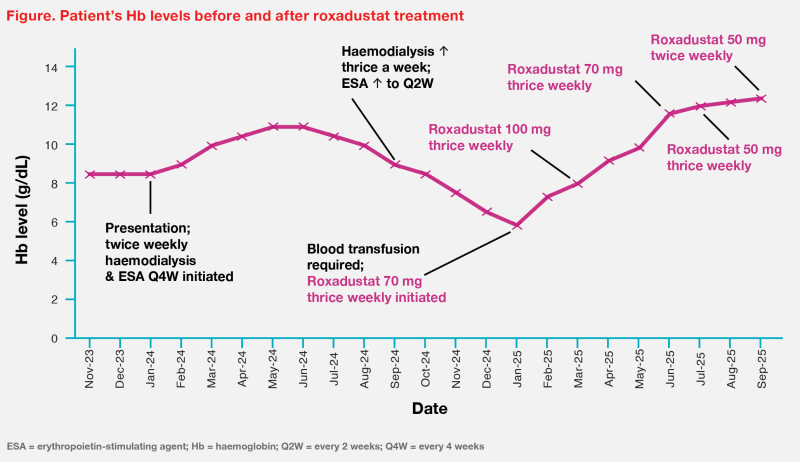
At the end of 2024, the patient’s serum creatinine level started rising and residual kidney function deteriorated further despite increased frequency of haemodialysis (thrice weekly). His Hb level continued to fall despite increased frequency (Q2W) of ESA therapy, dropping to a nadir of 5.8 g/dL in January 2025, which necessitated a blood transfusion. (Figure) During this period when the patient was anaemic, he experienced hypotension during dialysis, felt generally unwell and fatigued, and lacked appetite.
Treatment with roxadustat and outcome
As the patient remained unresponsive to the relatively high dose of ESA, he was switched to a different class of agent for anaemia treatment. Roxadustat, a hypoxia-inducible factor (HIF) prolyl hydroxylase inhibitor (HIF-PHI), was initiated in mid-January 2025 at 70 mg thrice weekly (starting dose based on his body weight of 55 kg). Initially, the patient’s Hb level increased only marginally to 7 g/dL and remained around that value throughout February 2025. Roxadustat dose was thus increased to 100 mg thrice weekly in early March 2025. This led to notable and sustained improvements in Hb level, which eventually reached >12 g/dL in July 2025. Roxadustat dose was stepped down to 70 mg thrice weekly in June, then 50 mg thrice weekly in July and eventually to 50 mg twice weekly in September 2025, during which the patient’s Hb level remained stable at around 12 g/dL throughout. (Figure)
Last seen in January 2026, the patient continued to receive roxadustat 50 mg twice weekly, and did not require any blood transfusion since taking roxadustat. His Hb level was stable at around 12 g/dL. He was feeling well and reported no roxadustat-related adverse effects (AEs).
Discussion
Anaemia is common in patients with CKD, and is associated with adverse clinical outcomes (eg, higher mortality, increased risk of CKD progression and cardiovascular [CV] disease). Timely and effective treatment is essential to normalize and maintain target Hb levels (range, 10–12 g/dL; >13 g/dL not recommended).1-3
Global guidelines such as Kidney Disease: Improving Global Outcomes (KDIGO) 2026 Clinical Practice Guideline for the Management of Anemia in CKD, UK Kidney Association Clinical Practice Guidelines for Anaemia of CKD, and Clinical Practice Guidelines for Management of CKD during Peridialysis in China (2025) recommend initiating anaemia treatment when Hb levels are <10.0 g/dL.1,3,4
HIF-PHIs, a novel class of agents, are an alternative to ESAs, especially in patients who are hyporesponsive to ESAs.1,3-6 Patients with ESA hyporesponsiveness are at increased risks for CV events, kidney failure, and death. At the same time, high doses of ESAs may contribute to the higher risk of stroke and other CV events associated with higher Hb targets in people with anaemia and CKD.1
Roxadustat, a first-in-class oral HIF-PHI for CKD-anaemia management, is recommended for non–dialysis-dependent as well as dialysis-dependent patients in leading guidelines across mainland China, as well as in guidelines of the Asia Pacific Society of Nephrology, in UK, Europe and recently, KDIGO.1-8
Roxadustat is a potent, orally administered, reversible HIF-PHI that activates the HIF pathway by mimicking the body’s natural response to hypoxia, specifically by stabilizing HIF-α, resulting in a coordinated erythropoietic response.7,9,10
Phase III studies have demonstrated roxadustat’s superior efficacy vs placebo and noninferior efficacy vs ESAs, with comparable safety profile.10-14
Study 808, which included 154 Chinese CKD patients not undergoing dialysis, found that those treated with roxadustat had a higher mean Hb level after 8 weeks vs those who received placebo (between-group difference, 2.2 g/dL; p<0.001). Treatment efficacy (ie, Hb correction and maintenance) was maintained during the 18-week open-label period. Compared with placebo, roxadustat also resulted in greater reductions from baseline in mean hepcidin levels (associated with greater iron availability; 56.14 vs 15.10 ng/mL).11
In study 806, 305 Chinese CKD patients on dialysis and epoietin-alfa were randomized to switch to roxadustat or remain on epoietin-alfa for anaemia management. At the end of 26 weeks, oral roxadustat was found to be noninferior to parenteral epoietin-alfa. In patients with elevated baseline C-reactive protein (indicating presence of inflammation), Hb responses in roxadustat-treated patients were not affected, while epoetin-alfa–treated patients had lower Hb responses. The hepcidin level associated with roxadustat resulting in improved mobilization of internal iron stores may have contributed to these findings.12
Despite increased incidence of hyperkalaemia in patients treated with roxadustat in the above trials, CV safety of roxadustat was comparable to that of ESAs and placebo in meta-analyses of global trials and long-term safety studies in Chinese patients. Roxadustat also showed similar incidence of other AEs vs ESAs or placebo. Guidelines nevertheless recommend monitoring of potassium levels and liver function in addition to Hb levels when using roxadustat.2,5,10-15
CKD anaemia is often undertreated. Injection hesitancy and the inconvenience of travelling to clinics to receive injections (for patients who are unable to self-administer) are among the deterrents for ESA treatment. The convenience of roxadustat’s oral administration is advantageous, especially in Hong Kong where home peritoneal dialysis is used as first-line dialysis modality.
References:
- Kidney Int 2026;109:S1-S99.
- Natl Med J China 2021;101:1463-1502.
- BMC Nephrol 2025;26:193.
- Chin J Nephrol 2025;41:788-810.
- Nephrology 2021;26:105-118.
- Nephrol Dial Transplant 2024;39:1710-1730.
- Evrenzo Package Insert, 4 September 2024.
- www.nice.org.uk/guidance/ta807.
- Am J Kidney Dis 2017;69:815-826.
- Chin Med J (Engl) 2025;138:1465-1476.
- N Engl J Med 2019;381:1001-1010.
- N Engl J Med 2019;381:1011-1022.
- Adv Ther 2021;38:5345-5360.
- Adv Ther 2023;40:1546-1559.
- Clin J Am Soc Nephrol 2021;16:1190-1200.
The above content is for medical education purpose supported by AstraZeneca Hong Kong Limited.
HK-12897. 31 May 2026. 
