An updated drug selection, stepwise prescribing, and a clear guide to what should—and should no longer—be on the prescription pad.
In medicine, as in all sciences, tradition without evidence is superstition—Sir James Black.
Knee
osteoarthritis (OA) remains among the top three musculoskeletal conditions encountered in outpatient clinics.
With an ageing population and rising obesity rates, the burden on primary care is growing. General practitioners (GPs) are the gatekeeper: the patient with knee pain will almost certainly go to GPs first, and the pharmacological choices GPs make at that first encounter have significant downstream consequences for pain control, functional outcomes, healthcare costs, and the risk of unnecessary procedures or surgical referral.
Yet audit data consistently shows a gap between evidence and practice. Many patients still leave their GP with prescriptions for glucosamine, a course of oral diclofenac without gastroprotection, or a referral for viscosupplementation—interventions that current major guidelines either do not support or explicitly recommend against. This article bridges that gap, drawing on the AAOS 3rd Edition Clinical Practice Guideline (2021) and NICE NG226 (2022), to give GPs a clear, practical pharmacological framework.
The non-pharmacological foundation
Before initiating drug therapy, it is vital to emphasise that both AAOS and NICE designate structured exercise and weight management as the highest-priority, most evidence-backed interventions for knee OA. These are not optional lifestyle “add-ons”—they are first-line treatments supported by robust evidence. Consequently, pharmacotherapy should be viewed as an adjunct to, rather than a replacement, for these core measures.
Nevertheless, pharmacological management remains a practical necessity alongside rehabilitation for many patients, making the selection of the right agents critical. Given the high prevalence of obesity and diabetes in the population, optimising metabolic care—including the strategic use of GLP-1 receptor agonists—should be considered. The introduction of these breakthrough drugs may serve as a potent “surgical adjunct,” potentially paving the way for reduced pain and superior patient satisfaction.
Stepwise pharmacological management
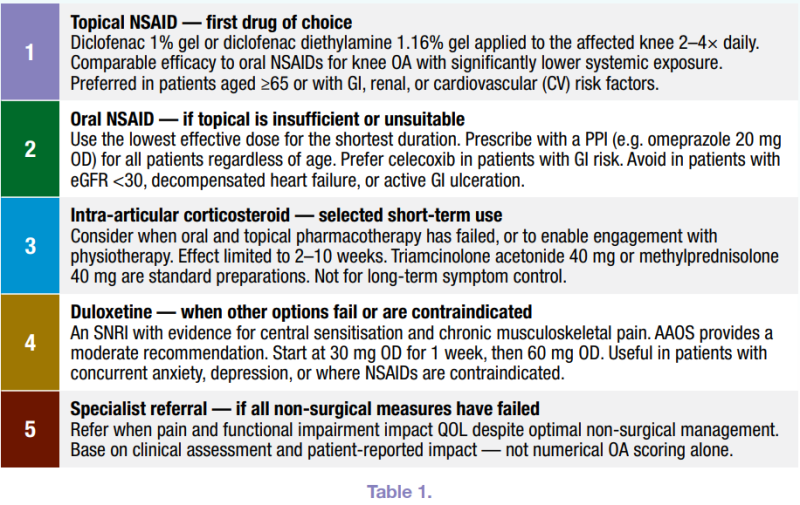
Current guidelines support a logical, stepwise approach to pharmacotherapy, escalating from topical to systemic agents and reserving injectable options for selected cases where oral and topical treatments have failed (Table 1).
Drug-by-drug: What to prescribe and why
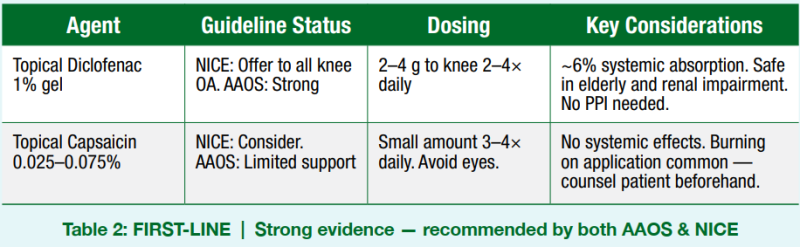
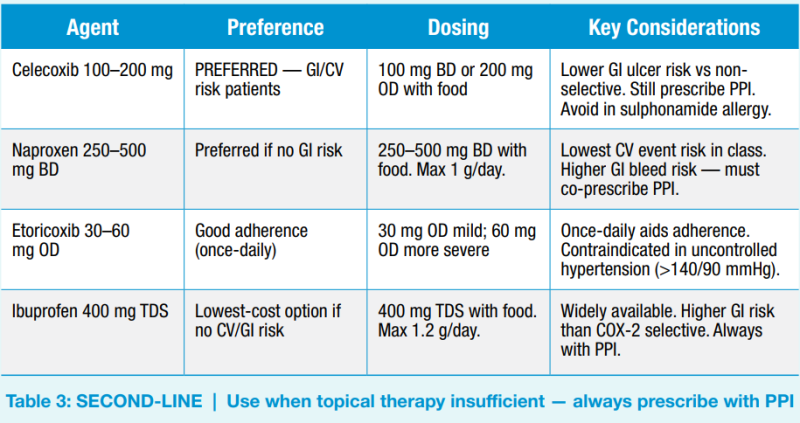
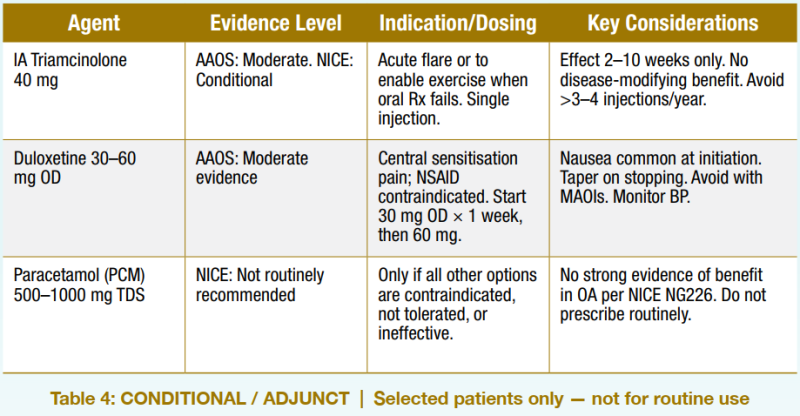
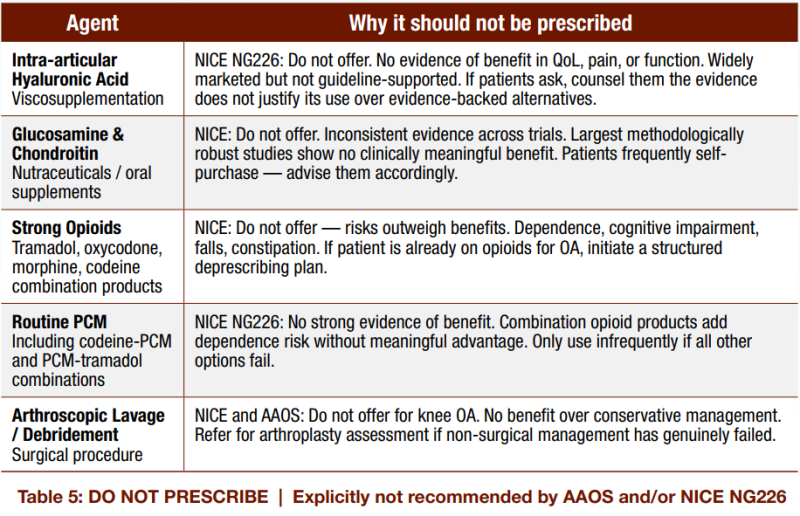
The following tables provide a practical summary of recommended and contraindicated pharmacological agents for knee OA management in primary care, with dosing, indications, and key prescribing considerations (Table 2-5).
A note on paracetamol: Reassessing a familiar default
Many GPs have long defaulted to paracetamol (PCM) as the ‘safe’ first-line analgesic for OA. NICE NG226 specifically challenges this. The guideline states there is no strong evidence of benefit for PCM in OA, and it should only be used infrequently for short-term pain relief when all other pharmacological options are contraindicated, not tolerated, or ineffective. This is a significant departure from previous guidance. In practice, this means PCM should not feature routinely on repeat prescription for a patient with chronic knee OA.
Special populations: Adjusting pharmacological choice
For patients >65 years old, topical agents become even more important as the primary and often only pharmacological intervention. The systemic risk profile of oral NSAIDs, GI bleeding, acute kidney injury, fluid retention, and CV events, rises with age, polypharmacy, and comorbidity. In this group, if oral analgesia is genuinely needed beyond topical NSAIDs and exercise, duloxetine may be preferable to an oral NSAID, particularly in those with concurrent pain-related low mood or anxiety.
In patients with chronic kidney disease (eGFR< 30), all NSAIDs—topical and oral—should be used with extreme caution or avoided. Even topical diclofenac carries measurable systemic absorption, and in the context of significantly impaired renal function this can precipitate acute kidney injury or worsen fluid retention. Intra-articular corticosteroid, with awareness of its effect on glycaemic control, remains a reasonable short-term option in this group alongside non-pharmacological management. Duloxetine should be dose-reduced and used cautiously in moderate-to-severe CKD.
In patients with type 2 diabetes requiring a corticosteroid injection, blood glucose should be monitored for 48–72 hours post-injection and advised accordingly.
Patients with recent active ischaemic heart disease on antithrombotic therapy
This patient group requires pharmacological vigilance. All oral NSAIDs, including COX-2 selective agents such as celecoxib and etoricoxib, carry a class-wide CV risk and are contraindicated in patients with established ischaemic heart disease (IHD), especially within the first 6–12 months following an acute coronary event such as MI, NSTEMI, or unstable angina. This contraindication is absolute in the acute phase and remains a strong caution indefinitely in those with ongoing coronary artery disease.
In this population, oral NSAIDs should not be prescribed for knee OA under any circumstances while the patient is in the active IHD phase or on dual antiplatelet therapy (DAPT).
For patients on antithrombotic therapy—whether single antiplatelet (aspirin or clopidogrel), DAPT, or anticoagulation (warfarin, DOACs such as rivaroxaban or apixaban)—the concern extends beyond CV risk. NSAIDs interact directly with antiplatelet mechanisms and significantly increase the risk of serious GI bleeding, particularly when combined with aspirin or anticoagulants. Even with PPI co-prescription, this risk remains clinically meaningful, and the combination should be avoided.
Topical diclofenac is the safest pharmacological option in this group, offering localised analgesia with minimal systemic absorption and no meaningful interaction with antiplatelet or anticoagulant agents at standard topical doses.
When topical therapy alone is insufficient, duloxetine 30–60 mg OD is the preferred oral analgesic adjunct in IHD patients, as it carries no CV contraindication and does not interact with antiplatelet or anticoagulant regimens. Intra-articular corticosteroid injection is a useful short-term option for acute flares; however, in patients on warfarin, the INR should be checked and stable before proceeding, and the injection should be performed under sterile conditions to minimise the already low but real infection risk in anticoagulated patients.
For patients on DOACs, no specific INR monitoring is required, but the timing of injections should ideally avoid peak anticoagulant effect windows. Physiotherapy and structured exercise remain the cornerstone of management in this group and should be actively encouraged, with cardiac rehabilitation teams involved where relevant. Strong opioids remain contraindicated regardless of IHD status.
Take-home message: A call to clinical action
The core message for modern practice is clear: Topical first, oral NSAIDs (with PPI) second, and opioids never. The evidence-based pathway begins with topical diclofenac as the primary pharmacological intervention, escalating to oral NSAIDs—supported by mandatory PPI gastroprotection—only when necessary. Intra-articular corticosteroid injections should be used judiciously for short-term relief, while duloxetine is reserved for patients experiencing central sensitisation or those with contraindications to NSAIDs.
Equally critical is the de-prescribing of outdated treatments. Strong opioids, viscosupplementation, glucosamine, and routine PCM should no longer be considered standard responses to knee OA. Persisting with these prescriptions exposes patients to avoidable side effects and unnecessary financial burdens, but most importantly, it delays access to the interventions that improve functional outcomes.
Adopting updated, evidence-based prescribing habits is one of the most effective ways a GP can improve the quality of life for this large patient population. The guidelines are definitive, and the evidence is compelling. The time to align clinical practice with modern standards is now. References: 1. Brophy RH, Fillingham YA. AAOS CPG Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), 3rd Ed. J Am Acad Orthop Surg. 2022;30(9): e721–e729. 2. National Institute for Health and Care Excellence. Osteoarthritis in over 16s: diagnosis and management. NG226. London: NICE; October 2022. 3. Bannuru RR et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular OA. Osteoarthritis Cartilage. 2019;27(11):1578–1589. 4. Conaghan PG et al. Evidence for the pharmacological treatment of OA: a long-term view. Rheumatology. 2019;58(Suppl 4): iv55–iv64.
Note: Associate Professor Dr Sanjiv Rampal is a Consultant Orthopaedic Surgeon at IMU University.